


PRACTICAL RECOMMENDATIONS
What is already known about this topic?
Importance of Pharmacogenetics: Pharmacogenetics is a crucial part of personalized medicine, allowing therapy to be optimized based on a patient's genetics.
Existence of STROPS: An international reporting guideline called STROPS (Strengthening the Reporting Of Pharmacogenetic Studies) already exists. It contains 54 items designed to ensure transparency, reproducibility, and completeness in pharmacogenetic research publications.
Quality Issues in Russia: Despite growing interest and an increasing number of publications in Russia, local studies often suffer from poor methodological detail, incomplete genetic data reporting, and a lack of attention to ethical and legal aspects of handling genetic data.
What is new in the article?
Adaptation for Russia: The authors propose a novel, adapted version of the STROPS checklist specifically tailored to the Russian regulatory and legal environment.
Integration of New Legislation: The checklist incorporates new requirements from upcoming changes in Russian legislation (Federal Law No. 86-FZ), which strictly regulates the collection, storage, and transfer of genetic data.
Journal Implementation: The article announces that the Russian journal "Pharmacogenetics and Pharmacogenomics" will mandate this adapted STROPS standard for all submissions starting in 2026, including a requirement for authors to submit a completed compliance checklist.
Practical Tool: It provides a detailed, bilingual (Russian/English) table that serves as a practical guide for researchers to ensure their manuscripts meet both international scientific and local legal standards before submission.
How can this affect clinical practice in the foreseeable future?
More Reliable Evidence Base: By enforcing stricter reporting standards, the quality of published Russian pharmacogenetic research will improve. This creates a more reliable evidence base for doctors to confidently use pharmacogenetic tests in their clinical decision-making.
Legally Compliant Integration: The focus on legal aspects (informed consent, data transfer bans, ethics approval) ensures that as pharmacogenetic testing moves into clinics, it will be done in a manner compliant with Russian law, protecting both patients and practitioners.
Development of Local Guidelines: Higher quality data will facilitate the creation of robust, evidence-based Russian clinical guidelines for pharmacogenetic testing, moving away from reliance solely on international data.
This article addresses the improvement of the quality of Russian pharmacogenetic studies through the adoption of the international reporting guideline STROPS (STrengthening the Reporting Of Pharmacogenetic Studies). In the context of the active implementation of pharmacogenetic technologies in clinical practice in Russia, the authors emphasize the need to ensure transparency, reproducibility and legal correctness of published pharmacogenetic studies as an evidence base for pharmacogenetics. We propose an adapted STROPS-based checklist tailored to Russian regulatory requirements, including ethical approval, genotyping methods, and restrictions on genetic data transfer. The Russian journal "Pharmacogenetics and Pharmacogenomics" plans to implement these standards in its review process starting in 2026. We believe the adoption of STROPS represents a crucial step toward enhancing scientific rigor and international recognition of Russian pharmacogenetic research.
PHARMACOTRANSCRIPTOMICS
What is already known about this topic?
Standard Approaches: Pharmacogenomics (studying the influence of genetic polymorphisms on drug metabolism) and pharmacometabolomics (therapeutic drug monitoring) are already actively used to personalize epilepsy therapy.
Therapeutic Challenge: Up to 60–70% of epilepsy patients require lifelong antiepileptic drug (AED) therapy, which is associated with a high risk of adverse reactions (teratogenicity, neurotoxicity, metabolic syndrome) and the development of therapeutic resistance.
Role of Epigenetics: It is known that some AEDs (e.g., valproic acid) can influence not only ion channels but also epigenetic mechanisms (histone deacetylase inhibition). However, a systematic approach to studying these effects has been lacking.
Potential of microRNAs: microRNAs were considered promising biomarkers for various diseases, including epilepsy, but their role in response to pharmacotherapy had been studied only fragmentarily.
What is new in the article?
Conceptualizing the Approach: The article comprehensively presents pharmacotranscriptomics as an independent and necessary "piece" of the multiomics puzzle in epileptology. It focuses on how AEDs change a patient's gene expression (transcriptome), not just the structure of their DNA.
New Mechanisms of Action: It shows that AEDs (valproates, carbamazepine, lamotrigine, etc.) can act as epigenetic modifiers, altering DNA methylation, histone modification, and microRNA expression. For example, this explains some of the anti-tumor or psychotropic effects of older AEDs.
Drug Repurposing: Systematizing transcriptomic data opens pathways for discovering new classes of drugs. For instance, understanding how valproic acid alters the expression of genes (BRD1, SCN3A) substantiates its use not only for epilepsy but also in oncology and for schizophrenia spectrum disorders.
Targets for New AEDs: The article proposes specific directions for creating new drug classes based on microRNAs (e.g., miR-139-5p agonists to overcome drug resistance).
Future Technologies: It describes modern methods (CRISPR-based screening, single-cell RNA sequencing) that will allow for the early detection of toxicity in AED candidates and the search for genes responsible for drug resistance.
How can this affect clinical practice in the foreseeable future?
New Diagnostic Panels: The emergence of "liquid biopsies" based on detecting circulating microRNAs in blood or saliva for early prediction of therapy failure or the risk of developing severe adverse reactions (e.g., metabolic syndrome).
Predictive Models: Implementation of algorithms that, based on a patient's transcriptome analysis, help a physician choose the AED with the highest probability of efficacy and minimal risk of toxicity for that specific individual (a shift from the "average dose for the population" to an "individual transcriptomic response").
Emergence of New Drug Classes: The development of fundamentally new molecules targeting not only ion channels but also the regulation of gene expression (e.g., drugs based on antisense oligonucleotides targeting microRNAs). This is particularly important for treating pharmacoresistant forms of epilepsy.
Refining Indications for Existing Drugs: Pharmacotranscriptomics will allow for more precise prescribing of AEDs in patients with comorbid conditions (e.g., choosing valproates when epilepsy co-occurs with bipolar disorder, considering its effect on the BRD1 gene).
Pharmacotranscriptomics is one of the important components of the multiomics approach to evaluating the efficacy and safety of drugs, along with pharmacometabolomics and pharmacogenomics. Pharmacotranscriptomics helps to understand how a patient's gene expression (transcriptome) changes in response to drug exposure (dose, duration of administration, etc.), especially during long-term use. This explains the researchers' interest in the pharmacotranscriptomics of antiepileptic drugs (AEDs), since lifelong AED therapy is required for up to 60-70% of people with epilepsy. This component of pharmacomultiomics can help in understanding the mechanisms of action of antiepileptic drugs, predicting treatment response, and identifying potential drug targets or biomarkers (for example, microRNAs). On the other hand, the prospects of pharmacotranscriptomics in the search for potentially new classes of AEDs are undeniable.
NEW TECHNOLOGIES
What is already known about this topic?
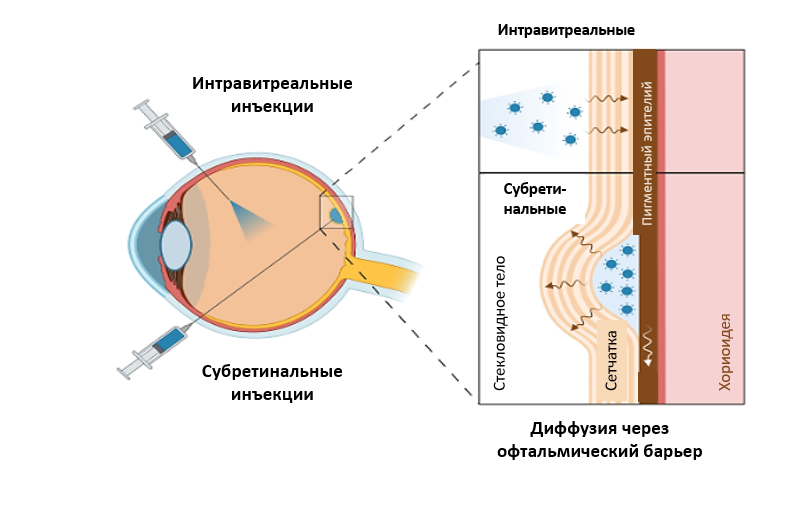
Limitations of Current Therapy: Current treatment for neovascular AMD (nAMD) requires lifelong, frequent intravitreal injections of VEGF inhibitors (e.g., ranibizumab, aflibercept). This creates a high burden on patients and the healthcare system, and carries risks of complications. For the dry form (geographic atrophy, GA), recently approved complement inhibitors (pegcetacoplan, avacincaptad pegol) also necessitate regular, ongoing injections.
Principle of Gene Therapy: The approach involves using viral vectors (primarily adeno-associated viruses, AAV) to deliver genes encoding therapeutic proteins directly to retinal cells. This aims to achieve long-term (years-long), endogenous production of the drug following a single administration.
Proof of Concept: The success of gene therapy for inherited retinal diseases (approval of voretigene neparvovec for RPE65 mutations) demonstrated the feasibility and safety of using AAV vectors in ophthalmology, paving the way for developing therapies for more common, multifactorial diseases like AMD.
What is new in the article?
An Up-to-Date Review of Drugs in Development: The article provides a detailed overview of the current landscape of gene therapy for AMD, systematically presenting data on key candidates at various stages of clinical trials (from Phase I to III).
Comparative Analysis of Strategies:
For nAMD: It details the three most advanced candidates:
Sura-vec (ABBV-RGX-314): Uses subretinal and suprachoroidal delivery to produce an anti-VEGF antibody fragment. Promising 2-year Phase I/IIa data are shown, with registrational trials (ATMOSPHERE, ASCENT) underway.
Ixo-vec (ADVM-022): Intravitreal administration producing aflibercept. Data from OPTIC and LUNA trials show an 86–92% reduction in injection frequency and a high proportion of injection-free patients (up to 69%). A Phase III trial (ARTEMIS) is starting.
4D-150: A unique dual-transgene construct (inhibits VEGF-A, -B, PlGF, and VEGF-C) delivered intravitreally. Phase II data show a 96.7% reduction in injection frequency, with Phase III trials (4FRONT-1/-2) initiated.
For GA: It presents drugs targeting key pathogenic pathways of the dry form:
JNJ-1887: Inhibits the complement system (MAC) by producing sCD59. Has Phase I data showing slowed GA progression, with Phase IIb (PARASOL) started.
OCU410: Modulates multiple pathways (lipid metabolism, inflammation, complement) by delivering the RORA gene. Phase I/II data show a 44% slowing of GA lesion growth.
4D-175: Aims to inhibit complement by delivering a truncated form of Factor H (CFH). It is in early-stage development.
Analysis of Delivery Routes and Immune Response: The article thoroughly discusses the advantages and disadvantages of different delivery methods (subretinal, suprachoroidal, intravitreal) in the context of transduction efficacy, inflammation risk, and technical complexity. It emphasizes the dose-dependent nature of inflammation and the importance of steroid prophylaxis.
How can this affect clinical practice in the foreseeable future?
A Paradigm Shift in Treating nAMD: If current Phase III trials (with data expected in 2026-2027) are successful, gene therapy could transform nAMD treatment from "chronic injection therapy" into a "single intervention with long-term disease control." This would radically reduce patient and healthcare system burden, improve compliance, and prevent vision loss from missed injections.
The First Pathogenetic Therapy for GA: For the first time, there is a real prospect of not just slowing the progression of GA but doing so with one or a few injections providing years of effect, in contrast to current drugs requiring continuous administration.
Personalizing the Treatment Approach:
The emergence of drugs with different mechanisms of action (blocking only VEGF-A vs. a broad spectrum of angiogenic factors vs. complement inhibition) will allow therapy selection based on the specific disease characteristics of a patient (e.g., JNJ-1887 might be preferable when nAMD and GA coexist).
The choice of administration route: For patients at high risk of inflammation, the subretinal route might be preferable despite its complexity, while for others, a less invasive intravitreal injection would be more acceptable.
New Challenges for Clinicians: Physicians will need to acquire new skills (e.g., performing suprachoroidal injections), manage new spectrums of adverse events (dose-dependent immune inflammation), and address ethical and organizational issues related to the high cost and accessibility of single-administration, but expensive, treatments.
Gene therapy is a promising approach for the treatment of age-related macular degeneration (AMD), aimed at overcoming the limitations of conventional anti-VEGF and anti-complement therapies. This review examines modern gene therapy strategies based on the use of adeno-associated viral vectors to deliver genes encoding proteins that inhibit angiogenesis and inflammation. Key gene therapy candidates for wet and dry AMD are discussed, including ixoberogene soroparvovec, ABBV-RGX-314, 4D-150, JNJ-1887, and others, along with their clinical trials. The advantages of gene therapy, such as reduced injection frequency and long-term efficacy, are highlighted, while challenges related to safety, immune response, delivery methods, and treatment accessibility are analyzed. The article provides a comprehensive overview of current advances and future prospects in gene therapy for AMD.
PHARMACOGENETICS STUDY

What is already known about this topic?
Treatment for multidrug-resistant tuberculosis (MDR-TB) often fails (with efficacy far below target levels) and is frequently complicated by severe adverse drug reactions (ADRs).
While pharmacogenetic markers (like NAT2 for isoniazid) are used for drug-susceptible TB, no such markers have been established for the modern MDR-TB regimens containing bedaquiline, linezolid, and fluoroquinolones.
It is known that enzymes like cytochrome P450 (CYP3A4, CYP3A5) and transporters (P-glycoprotein/ABCB1, ABCG2, SLCO1B1) are involved in metabolizing these key MDR-TB drugs.
What is new in the article?
New efficacy markers: The study identified two genetic markers strongly associated with poor treatment response (failure to stop bacterial excretion):
The CYP3A5 rs776746 (AA) genotype.
The ABCG2 rs2231142 (AA) genotype. Patients with this marker had a 0% rate of sputum conversion during the standard intensive phase.
New safety markers: The research found specific genetic predictors for common toxicities:
The ABCB1 rs2032582 (GG) "wild-type" genotype was linked to a 6-fold higher risk of neurotoxicity (peripheral neuropathy).
The ABCB1 rs1128503 (TT) genotype was linked to a 9-fold higher risk of gastrointestinal reactions.
Protective effect: The SLCO1B1 rs4149056 polymorphism appeared to be protective against arthralgia (joint pain).
How can this affect clinical practice in the foreseeable future?
Risk stratification: Clinicians could use these markers before starting treatment to identify patients at high risk of treatment failure (e.g., those with the ABCG2 AA genotype) or severe toxicity (e.g., those with specific ABCB1 variants).
Personalized regimens: High-risk patients could be selected for more intensive monitoring, prolonged treatment durations, or alternative drug dosing/selection to improve outcomes and prevent toxicities.
Development of a pharmacogenetic panel: These findings contribute to the potential creation of a specific test panel for MDR-TB, allowing for truly personalized medicine in managing this complex patient population.
Relevance. The treatment of patients with multidrug-resistant tuberculosis (MDR-TB) is often complicated by adverse drug reactions (ADRs) necessitating drug discontinuation. Its effectiveness falls short of target indicators and depends on a number of factors, including the patient's genetic profile. Pharmacogenetic markers for MDR-TB remain unstudied; their identification is expected to improve treatment outcomes through a personalized approach.
Objective. To determine pharmacogenetic markers associated with the efficacy and safety of treatment in patients with multidrug-resistant tuberculosis.
Materials and methods. A prospective cohort study included 40 patients with MDR-TB without HIV infection, receiving therapy with regimens containing bedaquiline, linezolid, and a fluoroquinolone in 2023-2024. A single 3-5 ml venous blood sample was collected from all patients irrespective of treatment duration. The presence of single nucleotide polymorphisms (SNPs) in cytochrome genes (CYP3A4, CYP3A5), P-glycoprotein (ABCB1), ATP-binding cassette transporter (ABCG2), and organic anion transporter (SLCO1B1) was determined using real-time PCR. These genes were selected based on literature and PharmGKB database analysis. Their association with treatment efficacy and safety parameters was assessed using univariate analysis, calculating odds ratios (OR) and 95% confidence intervals (95% CI).
Results. The following target polymorphisms were identified: SLCO1B1 (rs4149056, in 25.8%), ABCB1 (rs1045642 — in 75.0 %, rs2032582 — 72.2 %, rs1128503 — 77.8 %), ABCG2 (rs2231142 — in 24.3 %), CYP3A4 (rs2740574 — in 8.1 %), CYP3A5 (rs776746 — in 10.8 %). Treatment efficacy based on the criterion of sputum culture conversion was 89.3% (95% CI 72.0-97.1 %); the incidence of ADRs was 70 % (95 % CI 54.5-82.0 %), with neurotoxic reactions predominating (in 11 of 40 patients, 27.5 %). The CYP3A5 rs776746 AA genotype and the ABCG2 rs2231142 AA genotype were associated with the lowest rates of sputum culture conversion: 33 % and 0 % of individuals with each variant, respectively, compared to 100% in others, p < 0.01, OR 0.021 (95 % CI 0.001-0.77) and 0.083 (95 % CI 0.01-0.98). The risk of neurotoxic reactions was higher in the presence of the wild-type GG genotype of the ABCB1 rs2032582 gene (55.6 % vs. 16.0 % in patients with allelic polymorphisms, p = 0.034, OR 6.3, 95 % CI 1.2-33.3); the risk of gastrointestinal reactions was higher with the TT genotype of the ABCB1 rs1128503 gene (50.0 % vs. 10.0%, p = 0.045, OR = 9.0, 95 % CI 1.22-66.2).
Conclusion. Polymorphisms in the CYP3A5 (rs776746, genotype AA) and ABCG2 (rs2231142, genotype AA) genes associated with unfavorable treatment outcomes in MDR-TB patients were identified. Genetic predictors of neurotoxic and gastrointestinal reactions during the treatment of patients with multidrugresistant pathogen were determined.
CLINICAL PHARMACOGENETICS
What is already known about this topic?
Liver cirrhosis and its life-threatening complication, portal hypertension (leading to esophageal varices and bleeding), are a major cause of mortality worldwide.
Non-selective beta-blockers like propranolol are the standard therapy for reducing portal pressure and preventing variceal bleeding. However, the response is variable, and there is no clear algorithm for predicting efficacy.
Propranolol is metabolized by the CYP2D6 enzyme in the liver. Genetic variations (polymorphisms) in the CYP2D6 gene, such as the non-functional CYP2D6*4 allele, are known to affect the enzyme's activity and thus the metabolism of its substrate drugs.
What is new in the article?
Clinical Demonstration: This case series provides a direct clinical illustration of how the CYP2D6*4 polymorphism impacts propranolol's hemodynamic effect in cirrhosis patients.
The patient with the normal-function G/G genotype showed a dramatic 106.2% increase in portal vein blood flow velocity (MLPV), indicating a strong therapeutic response.
The patient carrying the non-functional allele (G/A genotype) showed a negligible 8.1% increase in MLPV on the same standard dose, indicating treatment failure.
Confirmation of Association: It strongly supports the association between carrying the non-functional CYP2D6*4 allele and a poor hemodynamic response to standard propranolol dosing.
Proposed Objective Criterion: The authors propose a specific, measurable criterion for treatment success: an increase in the mean linear velocity of portal vein blood flow (MLPV) of 20% or more from baseline, as measured by Doppler ultrasound.
How can this affect clinical practice in the foreseeable future?
Personalized Prescribing: It provides a strong rationale for implementing pharmacogenetic testing for the CYP2D6*4 polymorphism before starting propranolol therapy in patients with cirrhosis.
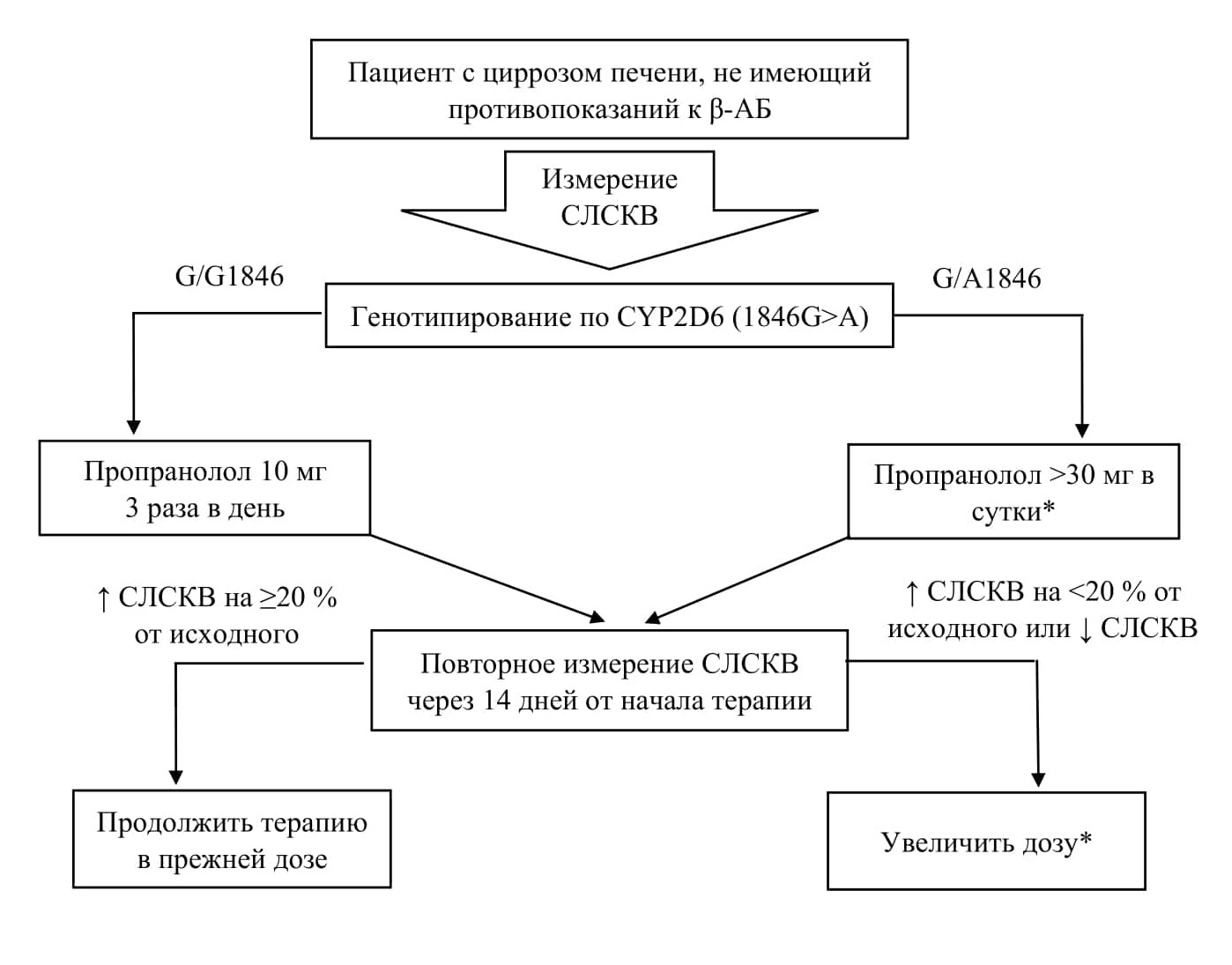
Actionable Dosing Algorithm: The study proposes a clear, practical algorithm for clinicians:
Patients with the normal (G/G) genotype can be started on the standard dose (30 mg/day).
Patients with the heterozygous (G/A) genotype (predicted poor responders) should be started on higher initial doses (>30 mg/day) to achieve a therapeutic effect, avoiding a period of ineffective, low-dose treatment.
Improved Prevention: This approach allows for early identification of patients unlikely to respond to standard therapy. By enabling proactive dose adjustment, it aims to optimize portal pressure reduction and more effectively prevent the high-risk complication of esophageal variceal bleeding.
The article presents two clinical cases of patients with liver cirrhosis and portal hypertension syndrome treated with the non-selective beta-blocker propranolol. The aim of this report is to demonstrate the impact of the CYP2D6*4 (1846G>A) polymorphic marker on the hemodynamic efficacy of the drug. In patient B. (heterozygous G/A1846 genotype), propranolol at a dose of 30 mg/day resulted in a slight increase in the mean linear velocity of portal vein blood flow (MLPV) — by 8.1%, which was considered an insufficient response. In patient G. (homozygous G/G1846 genotype), the same dosage regimen led to a pronounced increase in MLPV by 106.2%. Thus, carriage of the non-functional CYP2D6*4 allele is associated with lower propranolol efficacy. The feasibility of pharmacogenetic testing prior to prescribing beta-blockers to personalize therapy and prevent esophageal variceal bleeding is discussed.
What is already known about this topic?
DOAC Risks: Direct oral anticoagulants (DOACs) like rivaroxaban are the first-line therapy for preventing thrombosis in atrial fibrillation, but they can still cause hemorrhagic complications (bleeding).
Risk Factors: Bleeding can occur due to modifiable and non-modifiable factors. The HAS-BLED scale is used to assess risk, but it does not account for genetic factors.
Genetics and Metabolism: It is known that rivaroxaban is eliminated from the body with the help of the P-glycoprotein transporter (encoded by the ABCB1 gene). Mutations in this gene could theoretically slow down the drug's elimination.
What is new in the article?
Clinical Confirmation: The article presents a specific clinical case demonstrating a direct link between a genetic polymorphism and the development of hemorrhagic complications in a patient.
Specific Genotype: A patient with a low risk according to the HAS-BLED scale (2 points) and a correctly adjusted dose was found to have the mutant homozygous TT genotype of the ABCB1 (rs1045642) gene.
Mechanism: The authors show that this genotype led to slowed drug clearance: the patient's rivaroxaban concentration exceeded the norm (98 ng/mL, with a normal range of up to 87 ng/mL), which caused petechial rash, gingival bleeding, and gastric hemorrhages.
Diagnostic Value: The article substantiates the use of pharmacogenetic testing not so much for prediction, but for diagnosing the cause of a complication that has already occurred in patients with an apparently low risk.
How can this affect clinical practice in the foreseeable future?
Expanding Indications for Testing: Pharmacogenetic testing may become part of the diagnostic algorithm for patients with unexplained bleeding while taking DOACs, especially when clinical parameters (kidney function, age, dose) appear normal.
Personalized Drug Selection: In the future, if a patient has the mutant ABCB1 genotype, a physician might consider switching from rivaroxaban to another DOAC with a different elimination pathway (e.g., apixaban, as suggested by the authors) to minimize risks.
Moving Away from "Blind" Dosing: The article highlights the importance of transitioning from prescribing drugs based solely on clinical scales to a more personalized approach that considers the patient's genetic profile (even for medications taken lifelong with a wide therapeutic window).
Anticoagulant drugs have been used for a long time to treat diseases associated with an increased risk of thrombosis and thromboembolic complications. Based on many years of practice, the use of these drugs can lead to the development of hemorrhagic complications, which are also typical for the relatively recently introduced direct oral anticoagulants (DOAC). In the presence of a number of concomitant factors, hemorrhagic complications can develop even in patients with a low risk of bleeding according to the HAS-BLED scale. One of these factors is genetic. In the event of a mutation in the genes responsible for the biotransformation of DOAC, clearance slows down and the concentration of the drug in the blood serum increases, which can lead to a hemorrhagic complication. Pharmacogenetic testing can be used to determine the cause of a hemorrhagic complication while taking DOAC. This article presents a clinical example of a patient with complaints of hemorrhagic rash and gingival bleeding while taking DOACs with the presence of genetic risk factors for the development of hemorrhagic complications — ABCB1 (rs1045642) gene polymorphism –– mutant genotype TT, as well as the authors' discussions on the role of pharmacogenetic testing in diagnosing the cause of hemorrhagic complications while taking DOACs in patients with a low risk of bleeding according to the HAS-BLED scale.

ISSN 2686-8849 (Online)






































