


FROM EDITOR
What is already known about this topic?
Physicians generally have a positive attitude toward pharmacogenetic testing (up to 73% consider it useful).
Main barriers include: lack of knowledge, absence of testing in clinical guidelines, high costs, and long turnaround times.
Even when access is available, many physicians lack confidence in interpreting the results.
In Russia, access to testing is limited; costs range from 7,500 to 139,000 RUB, with turnaround times from 5 days to 16 weeks.
What is new in the article?
First-time comparative analysis of international (ESC, 2026) and Russian surveys (2022–2025), revealing the same structural gap between demand and actual access.
Physicians' personal experience with drugs metabolized by CYP2C19 or CYP2D6 increases their likelihood of recommending testing by 2–3 times.
Up-to-date assessment of testing availability in Moscow (using SLCO1B1 for statins), showing that most gene panels do not comply with international recommendations (CPIC, PharmGKB).
Evidence that even clinical pharmacologists do not yet routinely use pharmacogenetic testing.
Introduction of the new World-Class Genomic Research Center (Petrovsky National Research Centre of Surgery) as a key player in addressing these barriers under the Federal Scientific and Technical Program for Genetic Technologies (2019–2030).
How can this affect clinical practice in the foreseeable future?
Education: Mandatory training programs on interpreting pharmacogenetic tests for physicians (especially cardiologists and phthisiatricians).
Infrastructure: Possible government funding, test standardization, and reduced turnaround times.
Regulation: Inclusion of pharmacogenetic testing in clinical guidelines (both Russian and ESC), making it a mandatory rather than optional part of therapy.
Economics: Cost-effectiveness studies to justify routine testing for clopidogrel, statins, β-blockers, and antiarrhythmics.
Personalization: Testing may become truly accessible not only through private labs but also within the compulsory health insurance system — at least for drug groups with strong evidence.
This article investigates the factors hindering the widespread implementation of pharmacogenetic tests into routine clinical practice. Based on an analysis of international and Russian physician surveys (ESC, 2026; Russian surveys 2022–2025), the main barriers to the broad adoption of pharmacogenetic testing are examined. It is shown that despite a high level of physician readiness to use pharmacogenetic tests (up to 73 % of respondents), only one-third of specialists have actual access to them. Three key groups of problems are identified: a lack of knowledge and skills for result interpretation; insufficient infrastructure (high cost, long turnaround times, lack of standardization); and the absence of mandatory provisions in clinical guidelines. Overcoming these barriers requires a comprehensive approach, including improving the regulatory framework, training healthcare professionals, enhancing infrastructure, and providing economic justification.
CLINICAL PHARMACOGENETICS
What is already known about this topic?
P-glycoprotein (P-gp), encoded by the ABCB1 gene, affects the pharmacokinetics of many drugs and their passage across the blood-brain barrier.
The ABCB1 polymorphism (C3435T, rs1045642) is associated with altered functional activity of P-gp.
In patients with ischemic stroke (IS), "variant" genotypes CT and TT occur more frequently than the CC genotype.
ABCB1 polymorphism may be associated with resistance to clopidogrel and acetylsalicylic acid in IS patients.
What is new in the article?
Genotype frequencies of ABCB1 (C3435T) were determined in 120 Russian patients with non-cardioembolic IS: CC — 18.0%, CT — 56.0%, TT — 26.0% (total CT+TT — 82%).
For the first time, diabetes mellitus and overweight/obesity were significantly more common in CT+TT carriers compared to CC carriers (diabetes: 31.6% vs 18.2%, p=0.023; obesity: 36.7% vs 18.2%, p=0.003).
CC carriers had significantly higher blood leukocyte and neutrophil levels than CT+TT carriers (leukocytes: 9.2±2.3 vs 8.3±5.6, p=0.036; neutrophils: 6.2±2.9 vs 5.0±2.1, p=0.045).
No association was found between ABCB1 polymorphism and clinical features of IS or response to clopidogrel.
How can this affect clinical practice in the foreseeable future?
These findings may help prioritize the implementation of ABCB1 pharmacogenetic testing in patients with cerebrovascular pathology and concomitant metabolic disorders (diabetes, obesity).
ABCB1 testing could potentially be used to stratify patients at risk for adverse outcomes related to inflammatory response (leukocyte/neutrophil levels).
Further studies are needed on the impact of ABCB1 on the efficacy and safety of combined antiplatelet therapy (clopidogrel, aspirin, apixaban, rivaroxaban, dabigatran) in IS patients, which may eventually enable personalized treatment approaches.
Relevance. The study of the prevalence of ABCB1 polymorphic markers and the prediction of clinical, laboratory and demographic parameters in patients with ischemic stroke is a relevant area of pharmacogenetics and practical neurology.
Objective. To determine the frequency of ABCB1 polymorphism (C3435T, rs1045642) in patients with ischemic stroke and evaluate its association with clinical, laboratory and demographic parameters of patients.
Material and methods. The study group included 120 patients with non-cardioembolic ischemic stroke. Genotyping of ABCB1 polymorphisms (C3435T, rs1045642) was performed by polymerase chain reaction. An analysis of clinical and demographic factors and distribution frequencies of ABCB1 genotypes (C3435T) was performed.
Results. The CC genotype was verified in 18.0 %, CT in 56.0 %, and TT in 26.0 % of patients. The distribution of ABCB1 genotypes (C3435T, rs1045642) among patients with ischemic stroke complied with the Hardy-Weinberg law (χ²=1.81; p=0.18). When assessing the comparability of clinical and demographic characteristics and the results of genotyping for ABCB1 (C3435T, rs1045642), a statistically significant difference in the frequency of detection of diabetes mellitus and overweight in patients with ischemic stroke was noted. Diabetes mellitus and obesity were detected with a higher frequency in the group of patients carrying the CT+TT genotypes: in the presence of diabetes mellitus — 31.6 % versus 18.2 % (p=0.023); in the presence of excess body weight — 36.7 % versus 18.2 % (p=0.003). No statistically significant association with the clinical features of the course of ischemic stroke was found. Also, no characteristic differences were found between patients carrying the CT/TT genotypes (those who responded and those who did not respond to antiplatelet therapy with clopidogrel). When assessing the comparability of average quantitative laboratory parameters in carriers of the CC and CT+TT genotypes of the ABCB1 polymorphism (C3435T, rs1045642), it was revealed that in the general blood test, the average level of leukocytes and neutrophils was statistically significantly higher in the group of patients with the CC genotype.
Conclusion. The obtained data may influence the choice of priority for the implementation of pharmacogenetic tests both in cerebrovascular pathology and in other diseases.
What is already known about this topic?
The SLCO1B1 polymorphism (c.521T>C, *5 allele) is associated with reduced statin transport into hepatocytes, increased systemic concentration, and a higher risk of statin-induced myopathy.
In European populations, the frequency of the "slow" C allele ranges from 15–21%; the homozygous CC genotype increases the risk of myopathy more than 16-fold.
In Russia, the genotype frequencies of SLCO1B1 are: TT — 61%, TC — 32.5%, CC — 6.5%.
In the Uzbek population (patients with coronary artery disease and good statin tolerance), the C allele frequency is 15%, while in the complication group it is 38.5%.
What is new in the article?
First data on SLCO1B1 (c.521T>C) polymorphism frequency in the Kazakh population of East Kazakhstan: C allele — 18.0%, genotype TT — 73.6%, TC — 16.9%, CC — 9.6%.
CC genotype carriers showed a significant reduction in atorvastatin efficacy: total cholesterol at 6 months remained at 6.10 mmol/L vs 4.32 mmol/L in the TT group (41.2% difference).
A marked increase in creatine phosphokinase (CPK) activity was observed in CC homozygotes: at 6 months — 406.0 U/L vs 119.6 U/L in the TT group (239.5% difference, p<0.001).
The frequency of myalgia and muscle weakness in CC carriers at 6 months was 58.8% vs 4.6% in the TT group (χ²=23.31, p<0.001).
How can this affect clinical practice in the foreseeable future?
Testing recommendation: SLCO1B1 (c.521T>C) genetic analysis could be introduced in the Kazakh population to predict the risk of myopathy and reduced atorvastatin efficacy.
Therapy personalization: For homozygous CC genotype carriers, alternative statins (e.g., pravastatin or lower-dose rosuvastatin) or dose reduction with CPK monitoring should be considered.
Improved safety: Routine testing before statin prescription could prevent severe adverse effects (including rhabdomyolysis) in genetically predisposed patients of Kazakh ethnicity.
Cost-effectiveness: Identifying high-risk patients before initiating therapy may reduce costs associated with complication management and rehospitalizations.
Background. Prescription of dangerous and undesirable drug combinations occurs in healthcare systems of most countries worldwide. Among drugs with the highest risk in such combinations, statins are considered particularly hazardous due to their significant metabolic activity. In the healthcare system of Kazakhstan, this problem remains poorly studied, and the structure of genetic predisposition to adverse effects is unknown.
Objective. To determine the frequency of SLCO1B1 gene polymorphism in patients with coronary artery disease of the Kazakh population of East Kazakhstan and its association with the efficacy and safety of atorvastatin therapy.
Methods. A cross-sectional clinical-genetic study was conducted. The study did not involve any active intervention in the ongoing treatment of patients prescribed by physicians. Medical records containing prescription data from inpatient and outpatient settings were analysed. The presence of SLCO1B1 (c. 521T>C) polymorphisms of the OATP1B1 transporter protein was assessed.
Results. The study included 178 individuals (108 men and 70 women) aged 40 to 70 years (mean age 61.1±7.8 years). All patients were of Kazakh ethnicity. In the examined group of patients receiving statin therapy, a significant frequency of genetic variants associated with an increased risk of statin-related complications was identified. Significant differences in the frequency of clinical manifestations of drug-induced muscle adverse effects were observed for the SLCO1B1 gene in carriers of the homozygous CC genotype (χ² = 23.31, p < 0.001). A marked increase in creatine phosphokinase activity (3.39-fold, p < 0.001) and a reduction in atorvastatin efficacy were also observed.
Conclusions. In the studied Kazakh population, analysis of the SLCO1B1 (c. 521T>C) polymorphism can be recommended as a genetic marker of the risk of adverse reactions during lipid-lowering therapy with statins (atorvastatin), as this polymorphism reduces treatment efficacy and increases the risk of side effects.
What is already known about this topic?
20–30% of patients with schizophrenia do not respond adequately to antipsychotic therapy (pharmacoresistance, PR).
Genetic variability influences drug metabolism, adverse reactions, and treatment efficacy.
Polymorphisms in CYP2D6 and CYP2C19 are proven pharmacogenetic markers included in clinical guidelines.
Other genes (COMT, HTR1A, MDR1, CYP1A2, SLC6A4) have been discussed as potential markers of treatment response.
What is new in the article?
First comprehensive pharmacogenetic study in a Belarusian schizophrenia patient cohort (161 patients: 104 with PR, 57 without PR) covering 19 polymorphic loci in 15 genes.
Three polymorphic loci were significantly associated with PR:
CYP2D6 rs3892097 (A allele)
HTR1A rs6295 (CC genotype)
COMT rs4680 (G allele)
First description of pharmacogenetic risk profiles for PR in the Belarusian population:
G-/LL/T- (COMT / SLC6A4 / MDR1) → OR = 11.143
AG/AA (CYP2D6 / CYP1A2) → OR = 9.143
Combination of risk alleles from multiple genes significantly increases PR risk compared to single markers.
How can this affect clinical practice in the foreseeable future?
Personalized therapy: Identifying patients at high risk of PR before treatment initiation would allow timely prescription of alternative antipsychotics (e.g., clozapine) or dose adjustment.
Diagnostic panel development: The described genetic profiles could form the basis for the first specialized pharmacogenetic test for predicting PR in schizophrenia in Belarusian and possibly other European populations.
Preventive approach: Routine testing for CYP2D6, COMT, HTR1A, CYP1A2, MDR1, and SLC6A4 loci could prevent lengthy ineffective treatment courses, reduce hospitalization rates, and improve patients' quality of life.
Validation needed: These findings require confirmation in larger patient cohorts before routine clinical implementation.
Relevance. Despite the use of antipsychotic drugs is still one of the most effective treatment methods of schizophrenia, the 20–30 % of patients do not respond adequately to pharmacotherapy. This inefficacy may stem from genetic variability, which influences drug metabolism, adverse reactions, and treatment response, alongside gene-environment interactions. This study aimed to investigate the association between polymorphic gene loci and pharmacoresistant schizophrenia among Belarusian patients.
Objective. To study the relationship of a number of polymorphic gene loci with pharmacoresistance (FR) in patients with schizophrenia, residents of Belarus.
Methods. The study included 161 people with schizophrenia. The main group included 104 patients with no improvement when treating with two or more antipsychotics (including an atypical antipsychotic) for 6 to 8 weeks; the comparison group included 57 patients with positive response to pharmacological treatment of schizophrenia. Pharmacogenetic testing was performed using standard methods of nucleic acid isolation and PCR analysis. 19 polymorphic loci in 15 genes (CYP2D6, CYP2C9, CYP2C19, CYP1A2; MDR1, ANKK1, HTR1A, HTR2A, SLC6A4, HTR2C, COMT, MAOA, BDNF,
DRD2, UGT1A1) were genotyped. Statistical processing of clinical and genotyping data was carried out using the SPSS Statistics 20.0 program. The odds ratio (OR) and 95 % confidence interval (CI) were used as an indicator of the relationship between alleles and genotypes with the risk of developing PR.
Results. Comparison of the genotypes and alleles frequencies in the studied groups of patients with schizophrenia revealed an association of PR in carriers of alleles — A (CYP2D6, rs3892097) (χ2=4.124; p=0.042), G (COMT, rs4680) (χ2=9.006; p=0.003); AG genotype (CYP2D6, rs3892097) (χ2=6,647; р=0,01), CC genotype (HTR1A, rs6295) (χ2=5.522; p=0.019). Further analysis revealed an increase in the risk of PR when these alleles were combined with other gene loci. Patients with pharmacogenetic profiles A-/A(CYP2D6 / CYP1A2), (OR 2.926; CI 1.206–7.102); A-/B-/T(CYP2D6 / CYP1A2 / MDR1), (OR 4.833) had an increased risk of developing FR; CI 1,753–13,328); G-/L(COMT / SLC6A4), (OR 3,172; CI 1,500–6,709); G-/LL (COMT / SLC6A4), (OR 6,923; CI 1,900–25,227); G-/LL/T(COMT / SLC6A4 / MDR1), (OR =11.143; CI 2.415–51.414); CC/T(HTR1A / MDR1), (OR 2.564; CI 1.120–5.873).
Conclusion. A study using pharmacogenetic testing of residents of Belarus with schizophrenia revealed a significant association of the risk of PR with polymorphic loci of the genes CYP2D6 (rs3892097), HTR1A (rs6295), COMT (rs4680). An increased risk of PR was observed when the identified alleles were combined with polymorphic loci of the CYP1A2 (rs762551), MDR1 (rs1045642), and SLC6A4 (5-HTTLPR) genes. Pharmacogenetic risk profiles for the development of PR during antipsychotic therapy in patients with schizophrenia are described.
PERSONALIZED THERAPY
What is already known about this topic?
Methotrexate (MTX) is the first-line therapy for rheumatoid arthritis (RA), but adverse effects (AEs) occur in up to 72.9% of patients (GI reactions 20–30%, hepatotoxicity 10–15%, hematologic disorders 5–10%).
Polymorphisms in MTX metabolism genes (ABCB1, SLC19A1, FPGS, GGH, ATIC, MTHFR, DHFR) influence the drug's pharmacokinetics and pharmacodynamics.
Individual SNPs are associated with AE risk, but their predictive value is limited.
Pharmacogenetic testing can personalize therapy and reduce switching to expensive biologic agents.
What is new in the article?
First comprehensive analysis of 12 SNPs in 9 MTX metabolism genes in a Russian RA cohort (294 patients) using Multifactor Dimensionality Reduction (MDR).
Information-driven models (considering the biological role of genes) significantly outperformed automated models for predicting AEs.
A six-gene predictive model was developed with high diagnostic performance:
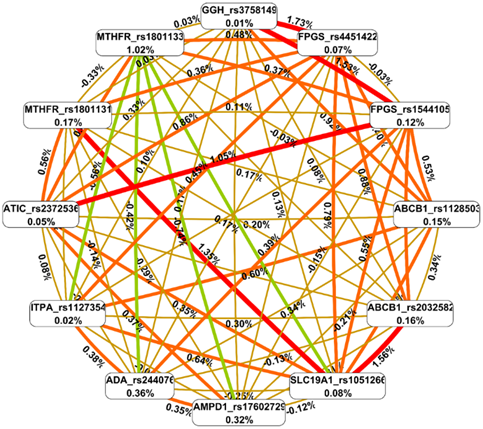
SLC19A1 rs1051266 + ABCB1 rs2032582 + FPGS rs4451422 + FPGS rs1544105 + GGH rs3758149 + ATIC rs2372536
→ sensitivity 91.5%, specificity 69.3% (p < 0.001, 10/10 cross-validation reliability).Epistatic (non-additive) interactions were identified between transport, polyglutamation, and adenosine pathway genes, contributing up to 1.73% to AE risk (vs 0.01–1.02% for individual SNPs).
A practical "if — then" rule and a registered computer program for predicting MTX AEs were developed.
How can this affect clinical practice in the foreseeable future?
Routine pharmacogenetic testing before MTX prescription could identify patients at high risk of AEs (sensitivity 91.5%).
Personalized first-line RA therapy: high-risk patients could receive alternative DMARDs or enhanced monitoring (liver function tests, blood counts).
Cost reduction: preventing MTX discontinuation due to AEs and avoiding expensive biologic/targeted therapies.
A ready-to-use domestically produced test system (TestGen LLC) and software for result interpretation are available.
Potential extrapolation to MTX therapy for other arthritides (undifferentiated, psoriatic).
Background. According to Russian and European clinical guidelines, methotrexate (MTX) is used for initial therapy of rheumatoid arthritis (RA), under regular medical and laboratory monitoring to prevent adverse reactions (AE). The incidence of AEs in MT reaches 72.9 %, with gastrointestinal reactions (20–30 %), hepatotoxicity (10–15 %), and hematological disorders (5–10 %) predominating. Hepatotoxicity requires long-term monitoring of liver function according to DILIN recommendations, while pulmonary complications (1–2 %) require immediate discontinuation of therapy. Polymorphisms of MT metabolism genes (ABCB1, SLC19A1, FPGS, GGH, ATIC, MTHFR, DHFR), by altering its pharmacokinetics and pharmacodynamics, determine individual tolerability of the drug. Pharmacogenetic testing enables the development of personalized approaches to RA therapy, reducing the risk of MT discontinuation and switching to expensive biologics.
Objective. To develop a pharmacogenetic model for predicting the risk of developing PD MT in patients with RA based on gene polymorphisms of key proteins involved in methotrexate metabolism.
Methods. The study included 294 patients with a confirmed diagnosis of RA who received MT monotherapy for 6 months. The associations between single-nucleotide polymorphisms (SNPs) of nine genes involved in MT metabolism and transport (ABCB1, ADA, AMPD1, ATIC, FPGS, GGH, ITPA, MTHFR, SLC19A1) and the development of PD were studied. Genotyping was performed by polymerase chain reaction (PCR) using domestically produced kits. A comprehensive statistical analysis was performed using multivariate dimensionality reduction (MDR) with 10-fold cross-validation, sensitivity and specificity assessment, and entropy analysis to identify epistatic gene interactions.
Results. PDs were recorded in 82 patients (27.9 %), primarily hepatotoxicity (17 %). Primary automated models involving 1–3 genes demonstrated low reliability, while data-driven models considering the biological role of genes demonstrated high predictive value. Five-gene and six-gene models, including polymorphisms of the transport systems (SLC19A1, ABCB1), polyglutamation (GGH, FPGS), and adenosine pathway (ATIC), proved optimal, with a maximum sensitivity of 91.5 % and specificity of 69.3 %.
Conclusion. A combined analysis of gene polymorphisms involved in MT transport and metabolism significantly improves the accuracy of predicting MT tolerance in patients with RA. A six-gene model combining the SLC19A1, ABCB1, GGH, FPGS, and ATIC genes demonstrated the greatest diagnostic value. The developed "if — then" predictive rule enables a personalized approach to therapy and can be used in clinical practice to predict the risk of MT-related PD.
DISCUSSION
What is already known about this topic?
Medication adherence in cardiovascular disease (CVD) patients is often low, which is associated with increased hospitalization risk and reduced quality of life.
Clinically significant gene polymorphisms affect drug pharmacokinetics, efficacy, and toxicity.
Pharmacogenetic testing can improve therapy efficacy and safety, but it is not yet routinely implemented in Russia.
Previous studies have shown a significant discrepancy between prescribed and taken medication lists in CVD patients, interpreted as a marker of low adherence.
What is new in the article?
First comparison of pharmacogenetic profiles of prescribed versus taken therapy in CVD patients at the cohort level (n=813 electronic health records).
A substantial mismatch was found between lists: 347 INNs prescribed, 253 INNs taken, with 435 INNs in total across both lists.
1,120 pharmacogenes associated with therapy were identified. The frequency of pharmacogenetic drug use reached 95–99%.
Statistically significant differences in the frequency of individual pharmacogenes between lists were found:
Prescribed drugs were more often associated with UGT1A9, UGT1A3, AGTR1, KIF6, SCAP (p<0.05).
Taken drugs were more often associated with ABCB1, NOS3, GNB3, ADRB1, ADD1 (p<0.05).
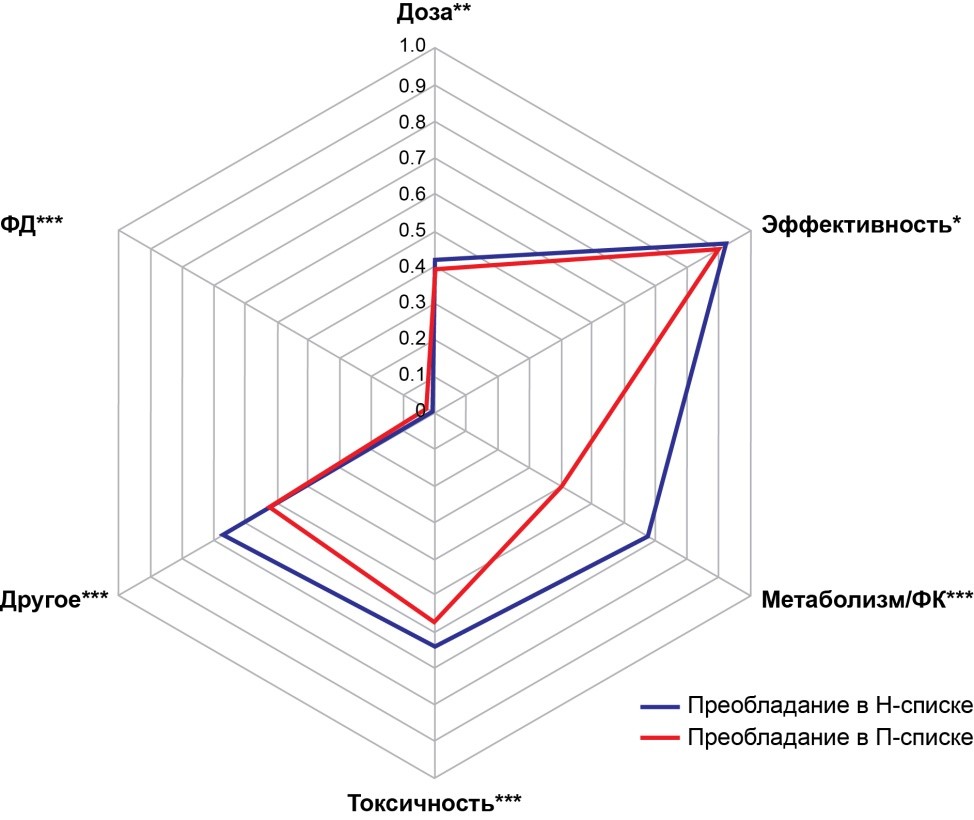
The group of pharmacogenes predominant in prescribed drugs surpassed the group from taken drugs in all parameters (dose adjustment necessity, effect on efficacy, metabolism/PK, toxicity), except for pharmacodynamics (p<0.05).
A new concept of "negative natural selection" of drugs is proposed, where drug-gene interactions act as the driving force.
How can this affect clinical practice in the foreseeable future?
Identifying pharmacogenetic causes of low adherence will enable personalized prescribing strategies for CVD patients.
Matching pharmacogenetic profiles of therapy with patient genetics may improve safety and treatment adherence.
Development of clinical decision support systems and pharmacogenetic panels tailored to regional and ethnic characteristics of the Russian population.
Creation of national recommendations for pharmacogenetic testing in patients with CVD and multimorbidity.
Monitoring of pharmacogenetic characteristics of prescribed therapy with data updates at least once every five years.
Objective. The study aimed to assess pharmacogenetic characteristics of prescribed versus taken pharmacotherapy in patients with cardiovascular diseases (CVD).
Materials and methods. A total of 813 electronic health records (EHRs) were selected from available electronic medical documents (n=8791) of CVD patients, using probability cluster sampling method. Unstructured text from the EHRs (n=813) was used to create a database characterizing gender, age, ICD-10 codes, prescribed and taken pharmacotherapy, international nonproprietary names (INNs), and pharmacogenes corresponding to each case of pharmacotherapy. Pharmacogenetic drugs and associated pharmacogenes were identified using database ClinPGx.org.
Results. Patients aged 62 years (IQR 56–68 years); 70.2 % men. The list of prescribed drugs comprised 347 INNs; the list of taken drugs comprised 253 INNs; both lists comprised 435 INNs, suggesting a mismatch between the lists. Numbers of INNs per document ranged from 1 to 23 for taken drugs (Me=6, IQR 3–9; n=385) and from 1 to 20 for prescribed drugs (Me=6, IQR 4–9; n=724), p > 0.05. The study identified 1120 pharmacogenes. Number of associated pharmacogenes per INN did not significantly differ between the lists of prescribed and taken drugs (1, IQR 0–7). However, the differences were found between the incidence rates of individual pharmacogenes. Pharmacogenes UGT1A9, UGT1A3, AGTR1, KIF6, and SCAP were significantly more often associated with prescribed drugs (p <0.05); ABCB1, NOS3, GNB3, ADRB1, and ADD1 were significantly more often associated with taken drugs (p <0.05).
Conclusion. The study demonstrated a mismatch between the pharmacogenetic profiles of prescribed versus taken pharmacotherapy in CVD. Drug-gene interactions may affect treatment adherence.

ISSN 2686-8849 (Online)






































